Conversations, either online or in person, are typically where my ramblings are conceived. I had such a conversation recently with someone who thought the COVID-19 closures of our society are ridiculous. His point was, we are all adults and therefore we should have the freedom to make our own decisions about our health. In a Darwinistic way, you could say what he says makes sense, that those who take the greatest risks are most likely to get sick and even die. I pointed out to this man, however, that if he gets sick, he will go to the hospital and then all these teams of caring frontline people will have to put their lives and the lives of their families at risk in order to save his. Not only that, he will be exposing a lot of people along the way, including his own family and the public. But his response took me by surprise. He said he did not care if he was responsible for killing everyone in the “healthcare industry,” because he hates them all (which, I guess, includes me).
The conversation above ended at that point, so I do not know what this man has experienced in his life that created this level of bitterness toward our entire healthcare system. But most people agree that there are problems within it, especially here in the US. Maybe, in these days of the COVID-19 global pandemic there is more benevolence toward our healthcare providers than in more typical times (save this one man I talked to), but we do know that there are problems and those problems will come to the surface once more when this is over.
There has been a copious amount of material written and views expressed about what is wrong with the healthcare system. These views come from the perspective of a variety of people including politicians, physician groups, patient groups, insurance companies, and others. They each carry a perspective and an agenda. It is like the proverbial story of the group of blindfolded people examining an elephant and describing what they feel.
I think I bring to the table a unique perspective as having a 38-year career in the practice of medicine as a PA, and now a high consumer of healthcare. Before I was sick, I rarely used the healthcare system as a patient and took no medications. The other thing I bring to the table is that I am very candid. I say things that are true, even if people do not want to talk about them. But with that said, the main point I am going to make in this article is not “The” problem with healthcare, but one of at least one hundred issues that could be raised.
The Dark Matter of Medicine
The brightest astrophysicists have no clue what dark matter (or dark energy) are, however, these entities make up 95% of the universe. But they do know it is there, mostly by its gravitational fingerprint on everything else. Modern medicine has its own version of dark matter, and that is the great complexities of our human body including the vast number of things we know and the humble admiration for the even greater things we do not.
The science of medicine was built on the shoulders (to loosely borrow an idea from Newton) of giants in the field of biomedical research. We have come so far in the past one hundred years that it is mind boggling. It was less than 100 years ago when penicillin was discovered, which revolutionized medicine at that time. However, seeing an area of bacterial clearing on a petri dish around mold (the essence of how penicillin was discovered) is at the level of a middle school science fair. We are light years beyond that now.
This profound knowledge of biological systems also exposes the vastness of the biological universe that we still do not understand and that is the real dark matter of medicine. As far as we have come, we are only standing waist-deep on the shores of the Pacific Ocean looking out into the vastness of the abyss. This has never been clearer to the public than during the COVID-19 pandemic, when there is frustration that we do not know more about this novel (new) virus, and yet, amazed about how much we do know about viruses in general.
We have long ago gathered the low-lying fruits of the apple tree (such as discovering penicillin) and the cost of discovery and the complexities there-of grow exponentially going forward. This is one of the major economic forces in medicine, where the cost of a medication, which requires a one-billion-dollar investment and a decade and a half of time to finally reach the market. Since insurance companies have to carry the brunt of this increased cost, they cut corners in other areas, such as paying for the time a provider spends with the patient. This indirect facet frustrates both the patient and the provider, but that’s another story.
I want to summarize how this issue of the dark matter of medicine directly impacts the practical application of medical care and the healthcare system from the provider’s and patients’ perspectives.
Providers Perspective. A high school friend’s uncle was a physician. This was 1973 and this uncle was still practicing, and I think he was well into his nineties. He started his medical practice around 1905, at the tender age of 20. In those days, premed and medical school could be abbreviated because the pool of knowledge in medicine was vastly smaller than today. Not only could he start his career without a residency (and without debt) but once in practice, making a diagnosis and treatment was relatively simple. He could see a patient in ten minutes and focus nine of those minutes on more social aspects of the visit such as asking the patient about their family, their work, and even hobbies.
It was also much easier for a provider to make a good living one hundred years ago than today because you could see forty or fifty patients per day as the diagnosis and treatments were so simple and the documentation of the visit, if any, were reduced to a one sentence scribble. The costs of running a practice were vastly lower than today as well. I will not diverge into another facet and that is the laborious problem of documentation in medicine, to satisfy the malpractice lawyers and the insurance companies. That is a facet within itself.
Even fifty years ago, seeing a patient was like someone coming in saying their bike was not working right and you have 15 minutes to figure it out and fix it. But now, it is more like a patient arriving in a very complex Boeing 747 and tell you that it isn’t working right, and you still have only 15 minutes to make the diagnosis and treatment plan. For example, in my area of medicine, fifty years ago a patient would go see their doctor and say they suffer from headaches and their doctor would say, “You are not handling your stress well. Here’s a stress pill.” However, we know vastly more about headaches today. A good headache clinician knows that there are about 110 different headache types and it takes time to go through the history very carefully and examination to arrive at a proper diagnosis and treatment plan. This plan will be based on the complex pathophysiology of headache that involve deep brain structures and a complex cascade of events that play out on the outer membranes of the brain.

But I want to focus on the part of the dark matter which, like in the astrophysics counterpart, is the vastness of what we do not know about disease and treatment.
Patient’s Perspective
I first entered the world of healthcare when I took a job in a hospital while I was in college studying premed. One part of the healthcare provider (used in the broadest sense, including nurses, nurse assistants, and etc.) culture I observed was that patients are considered as not knowing much and have the tendency to be hysterical. This same attitude continued to be part of my own medical education, both in the PA program I was in and with the medical students that I shared space with. It is a running joke about how stupid and hysterical patients can be. This attitude made me feel uncomfortable even then.

I had one professor during my PA school experience that was the exception to this culture. He was a psychiatrist and taught our psychiatry medicine lecture series. He was a nice guy and was the spitting image of John Denver. He started each class by telling a fascinating patient story to illustrate a diagnosis or issue that he wanted to discuss that morning.
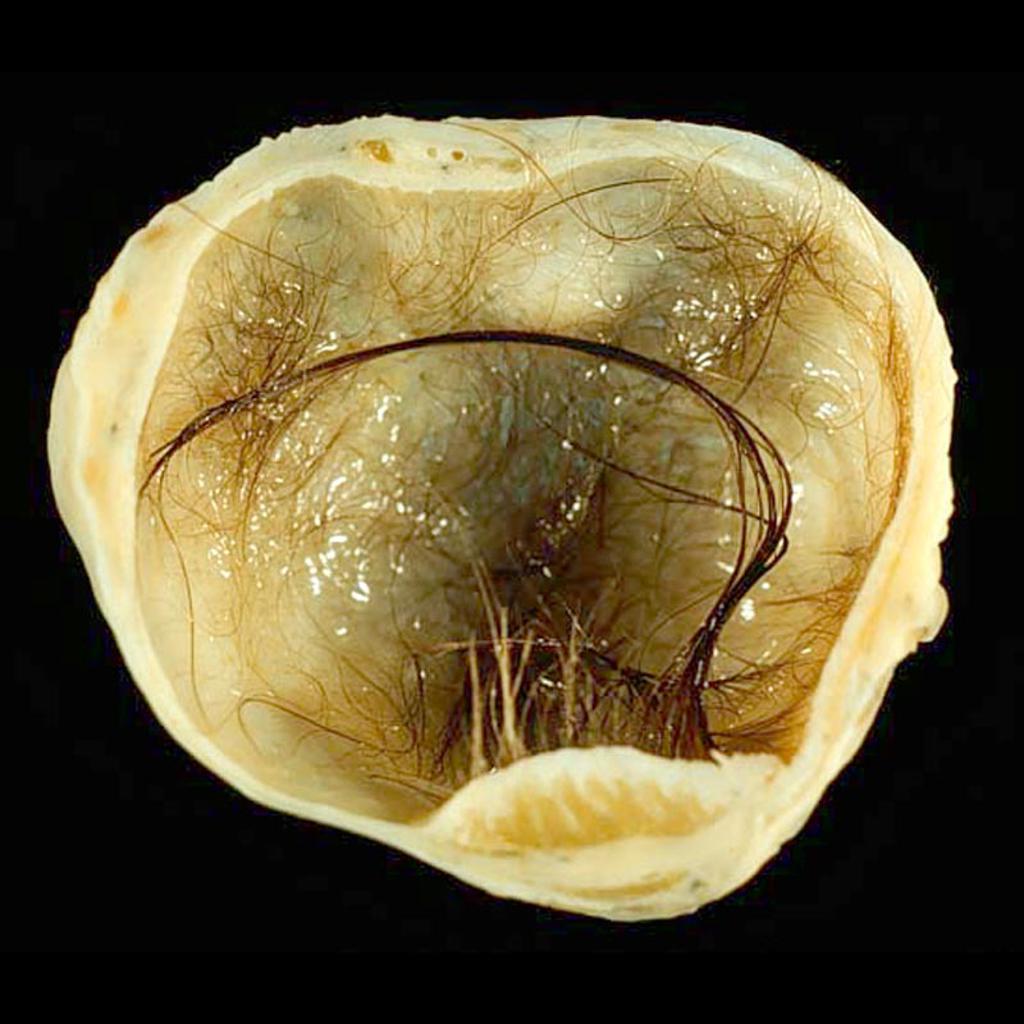
One day he came in and sat on the front of his desk. He smiled and then started to speak, “The Internal Medicine Clinic (at the University of Kentucky) sent me a patient one day with the diagnosis of ‘delusions of being a cat.’ I scratched my head as I had never heard of such a thing, although I guess it is possible to have delusions about anything. This well-dressed lady came into my office and took a seat on my couch. I asked her, ‘So, what’s going on,’ to which she replied, ‘I’m coughing up hair balls.’ ‘Really?’ I asked. Then I asked her, ‘Can you cough up one for me?’ She answered, ‘Sure.’ I handed her a box of Kleenex and she started coughing and then spit out a wad of long red hair. It was incredible! I immediately sent her to our pulmonology clinic, where she was eventually diagnosed with a bronchial teratoma, which is a type of tumor that can grow hair, fingernails, or even teeth. Her doctor had never asked to see the hair balls but had assumed that she was hysterical.”
The point that this psychiatrist wanted to make was to treat patients with respect by listening to them and believing them, even if you can’t explain their complaint. While their self-diagnosis may not be correct, their observations of something being wrong is accurate. Because the patient is not medically trained, they may not know the right terminology or understand the biochemistry of our bodies, but most the time their observations are based on something real. He also pointed out that it is quite rare that a patient is truly hysterical and just makes up symptoms.
Personal Story
One of the rabbit holes I refuse to go down, when it comes to my own health, are the “what ifs.” What if I had gone to see my doctor two months earlier? I did go in four months before I became ill and asked specifically for a Multiple Myeloma work up, which was done and was negative. If I had gone in as soon as I had symptoms, I would still have Multiple Myeloma but probably not the degree of kidney failure. I will try to explain why I did not go in. But this is not about me and my story but the much broader point that I am trying to make about this one facet of health care.
March is Multiple Myeloma Awareness Month. I saw a sign one day point this out and then listing the ten signs and symptoms of Multiple Myeloma. Oddly, I have never had one of the ten. That is why this was so confusing for me, even as a medical provider. My early symptoms were all neurological, coincidentally the field I have spent my entire career in.
At first, I thought I must have ALS and I was in no hurry to see my doctor because I knew he would only send me to the neurologist. It would take three months to get in to see the neurologist and then he would end up telling me I was going to die and there was nothing he could do about it. So, I told Denise to prepare to become a widow and I continued my life the best I could, working as hard as I could in my own clinic and taking care of our house in case I was gone.
My neurological symptoms continued to spread from my motor system into my autonomic system. Besides twitching and myoclonus all over, I started having difficulty swallowing and defecating. But the strangest one, which I still have although less intense, is that if I coughed or sneezed I would have about 30-50 places in my body go into spasm. They are clearly visible to the observer. However, I never developed the muscle wasting that you typically see with ALS. This created a very confusing picture for me and for all my medical providers since.
I will be honest and say that my hesitation about going to my doctor at the early point was that I knew that these symptoms didn’t fit any neurological disease state and I was afraid I would be labeled hysterical or some kind of whiner. Then I developed a new symptom, a sudden onset of severe neck pain and numbness down my arm. For that reason, I went to see my doctor.
When I saw my doctor, I told him about my neck pain, but also talked about my bigger problem of the neurological symptoms. I told him that if I forced a cough my entire body goes into spasms and asked if he wanted to see it. He said no. Then he focused on my neck pain and told me that my neurological symptoms were “stress” related to my neck pain. I knew better, but it was what I had feared.
To make a long story short, he did order a CT scan for my neck and to get a CT scan, over the age of 60, you must get renal function tests. My renal function tests came back extremely abnormal and I was sent from radiology directly to the ER and then to a telemetry unit at Peace Health in Bellingham.
Since that time, I have met countless medical providers who had no interest in seeing my twitching or spasms (which are impossible to fake) and have hinted over and over that either I’m making up the symptoms (hysterical) or they just shrug their shoulders and don’t want to talk about it. But these neurological symptoms are so severe, although slightly better now, that a year ago I was becoming suicidal (considering all the things I was facing, but these 24-7 neurological symptoms being the worst).
It wasn’t until I went to the Seattle Cancer Care Alliance did anyone ask to see the twitches. It was a PA in the bone marrow transplant unit. She was impressed and confused by the physical signs that no one could fake. But before that, and since, I’ve spoken to at least ten physicians who have no interest in seeing these twitches or talking about them, and if I keep bringing it up, they suggest I’m being hysterical.
I have read every study published anywhere in the world on neurological symptoms of renal failure. I found only one paper that presented three patients who had renal failure and this type of twitching all over their bodies, but all three also had seizures, so it was not the same syndrome. But that paper confessed that no one knows why neurological injuries can happen during renal failure and that it could manifest in ways that have not been reported.
My point here, is that there is a problem when you teach the medical providers that they know everything about medicine and anything that does not fit within that vast knowledge base, isn’t real. I hope that I knew better than this when I was a medical provider. I tried my best to listen to my patients and take what they were saying seriously. I even wrote an article for a national magazine back in the nineties on this very subject, titled, No Silly Symptoms.
I remember one of my patients who had a rather complex group of symptoms that I could not explain, nor could any of the doctors she had visited. However, I kept telling her that I think it is real, but it is something that has not been described yet in the medical literature. During this time, she visited the ER in Bellingham and there the physician told her (once again) that she was just hysterical, and she was not having the symptoms she was claiming to have. She told him, “Mike Jones believes they are real” to which she said that he replied, “Mike Jones is nothing but a PA and an idiot.” I didn’t know the man, nor did he know anything about me.
But this attitude of out of sight out of mind, or if I didn’t study it in medical school, it isn’t real, creates a lot of dissatisfaction among patients. It would be so much better for a provider to say something like, “That must be terrible. I don’t know what it is, but I will do some reading to see if I can figure it out. If I can’t, I would be happy to send you to a specialist and see if they can figure it out.”
This change in our healthcare delivery culture requires the patient to not demand simple and certain answers but to understand the limit of our medical knowledge without thinking the provider is an idiot or does not care about them. It also requires the provider to understand their own limitations and to drop this preconceived idea that most patients are dumb and hysterical. It means listening. It means looking at the signs (the visible manifestation of symptoms) and taking the patient seriously and be honest enough to say, “I don’t know” and to be motivated enough to seek answers by study or referral.
Mike

Leave a comment